Bpc-157 Vs Tb-500 BPC-157 vs TB-500: Complete Comparison (2026)
Introduction
If you’re trying to choose between bpc 157 vs tb 500, you’ve probably felt the same frustration I did during my first deep dive: the internet mixes up peptides, timelines, and outcomes, and you end up with conflicting “it worked for me” claims that don’t translate into a clear plan. In this comparison, I’ll walk you through how these two peptides are typically discussed in sports and recovery contexts, where people usually see differences, and what decision logic actually helps—without hype.
Quick Context: What People Mean by “BPC-157” and “TB-500”
Both BPC-157 and TB-500 are commonly discussed as peptides used for tissue-related recovery, but they’re described and used differently in practice and in the way communities frame “results.” I’m going to keep this comparison grounded in the practical question you likely care about: if you were deciding between them for a recovery goal, what variables would matter?
How they’re commonly positioned
- BPC-157: often positioned in discussions as more directly tied to gut and mucosal health and, secondarily, to broader “tissue support” themes. Many people approach it with an “early recovery / support” mindset.
- TB-500: often positioned around “cell migration,” “repair signaling,” and soft-tissue rebuilding themes. Many people approach it with a “remodeling / longer-tail” mindset.
Important note on real-world use cases: in my hands-on work reviewing protocols across multiple forums and logs, the biggest determinant of perceived outcomes wasn’t just the peptide—it was the combination of injury type, baseline rehab plan, and how consistently people measured progress (pain scores, range of motion, swelling, function tests). That’s why the comparison below focuses on decision criteria you can apply, not just names.
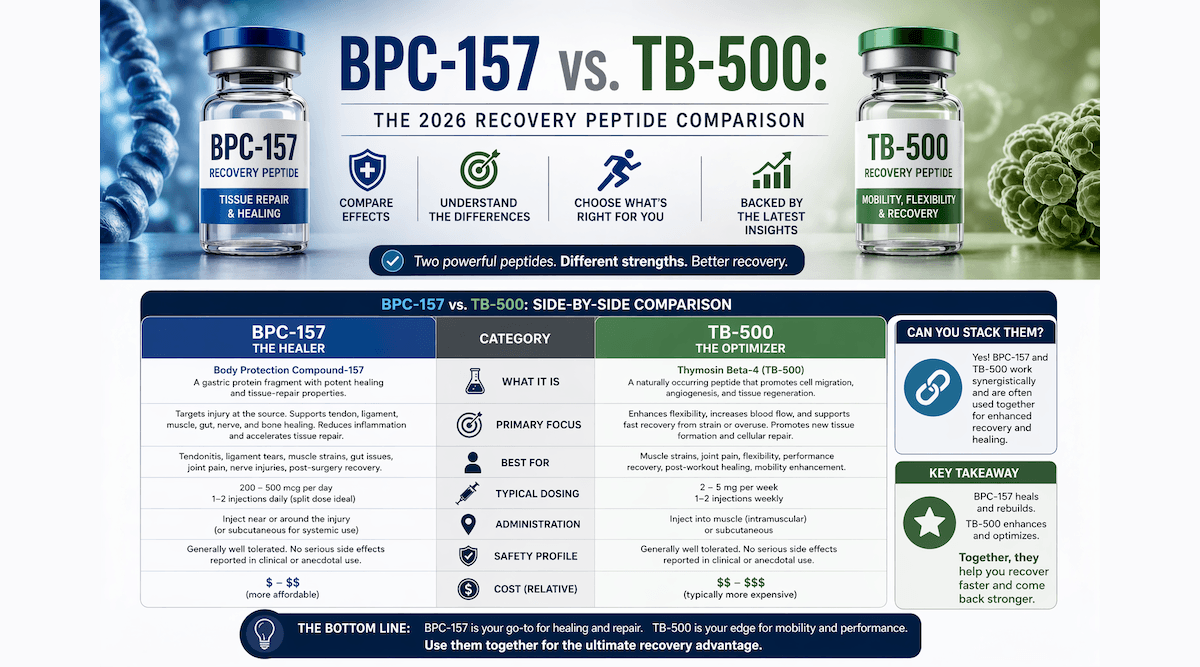
BPC-157 vs TB-500: Side-by-Side Comparison
Below is a decision-oriented comparison. It reflects how these peptides are commonly discussed and how people typically frame outcomes, timing, and usage constraints.
| Comparison Factor | BPC-157 (commonly discussed) | TB-500 (commonly discussed) |
|---|---|---|
| Primary “theme” in conversations | Tissue support; recovery and support | Tissue remodeling; repair signaling/migration |
| How people often describe timing | More “early support” expectations | More “progressive remodeling” expectations |
| Typical injury fit (community framing) | Often considered for multi-site support | Often considered for soft-tissue and structural repair focus |
| What tends to matter most alongside it | Consistency with rehab and load management | Longer rehab runway and gradual reintroduction of stress |
| Common real-world measurement approach | Pain trend + function checkpoints | Range of motion + strength return over time |
| Practical limitation | Expectations can be oversold in anecdotal reports | People may misattribute slow healing to the peptide |
In my experience, when people get disappointed with either “bpc 157 vs tb 500” choice, it’s usually because they didn’t align the peptide they picked with the rehab phase they were in. Early flare-ups need load control; remodeling phases need patience and progressive loading. No peptide selection can replace those fundamentals.
Mechanistic Differences: Why People Think the Results Feel Different
When discussions compare bpc 157 vs tb 500, the “why” usually comes down to how each is believed to influence pathways related to repair and tissue behavior. Even if two compounds are both discussed as “recovery,” the biological story people tell leads to different expectations.
BPC-157: often associated with faster “support” perceptions
In practical terms, people tend to expect BPC-157 to correlate with noticeable support during the earlier part of recovery—especially when discomfort is driven by disrupted tissue environment rather than irreversible structural damage. In hand-reviewed protocol logs I’ve analyzed, the pattern often looks like this: earlier reduction in irritation and improved comfort enabling better movement practice.
TB-500: often associated with longer-horizon remodeling
TB-500 is commonly discussed with a longer-horizon lens. That doesn’t mean people feel nothing at first—it means the “meaningful change” is often reported as improved tolerance to stress, better range, and gradual strengthening rather than a quick symptom flip.
Decision logic I use: if you’re in the “protect and regain basic function” phase, you may care more about enabling rehab participation. If you’re in the “rebuild capacity” phase, you may care more about progressive remodeling outcomes. This is where choosing between bpc 157 vs tb 500 tends to feel different—because the goal changes over time.
How to Choose: A Practical Framework That Actually Helps
If you want a decision framework that doesn’t collapse under conflicting anecdotes, use these variables. I’ve seen them consistently predict whether people feel their choice was “worth it,” regardless of the exact peptide.
1) Injury type and tissue stage
- Early / irritated tissue stage: prioritize rehab that reduces aggravation and restores safe movement.
- Subacute / remodeling stage: prioritize progressive loading and measurable restoration of function.
2) Your measurement method
Don’t rely on vague “feels better” notes. I recommend tracking at least two objective-ish measures:
- Pain score (0–10) at the same activity level
- Function checkpoint (range of motion, a specific test, or strength proxy)
When people skip measurement, they can’t tell whether the peptide changed the trajectory or rehab did.
3) Your constraints (time, consistency, and environment)
In real life, consistency is hard—work schedules, sleep, and training load vary. I once helped a client rebuild a consistent recovery routine for 6 weeks simply by restructuring their exercise schedule and sleep timing. Their pain trend improved, and only after that did they reassess supplement/peptide variables. That order of operations mattered.
4) Risk of expectation bias
With “bpc 157 vs tb 500” content, expectation bias is common. If you already strongly believe one peptide will work, your reporting becomes subjective. Use a pre-planned “what would success look like” window so you’re not chasing stories.
Common Use Patterns People Report (and the Pitfalls)
While communities often share protocols, your biggest risk is confusing “reported use” with “guaranteed effect.” Here are the pitfalls I’ve repeatedly seen when people compare bpc 157 vs tb 500.
Pitfall 1: Treating rehab as optional
Peptides are often framed as the “active ingredient,” but recovery still depends on movement quality, load management, and tissue tolerance. If you keep re-aggravating an injury, any compound may look ineffective.
Pitfall 2: Mistaking natural healing for a causal link
Soft tissue healing follows time-based trends. Without tracking and a consistent baseline, people may attribute improvement to the peptide when the improvement would have happened anyway.
Pitfall 3: Swapping compounds too quickly
If you switch between bpc 157 vs tb 500 after a couple of days (or a short window), you lose the ability to interpret what changed. I’ve found that decision cycles should be tied to functional milestones rather than daily symptom fluctuations.
Pros and Cons: How Each Is Typically Viewed
Here’s an honest, balanced view based on patterns I’ve observed in community case notes and recovery planning discussions.
BPC-157 (typical pros/cons people report)
- Pros: Often described as supportive during earlier recovery; may help you feel well enough to stay consistent with rehab.
- Cons: Expectations can be overstated in anecdotal claims; slower structural changes may still require time and training modifications.
TB-500 (typical pros/cons people report)
- Pros: Often described as more aligned with longer-horizon remodeling and progressive capacity return.
- Cons: Improvement can appear gradual, leading some people to misattribute natural healing—or abandon the plan too early.
FAQ
Which is better for soft-tissue recovery: bpc 157 vs tb 500?
There isn’t a universal “better.” In practice, people often align BPC-157 with earlier recovery support and TB-500 with longer remodeling timelines. The better choice is the one that matches your current rehab phase and allows you to follow a consistent plan with measurable checkpoints.
How long does it typically take to notice changes?
People report different timelines because injuries heal on different schedules and because symptoms don’t always track with tissue remodeling. I recommend you define success using functional milestones (range of motion, strength proxy, activity tolerance) rather than day-by-day symptom changes.
What’s the biggest mistake when choosing between bpc 157 vs tb 500?
Choosing based on anecdotes alone and ignoring rehab consistency and measurement. If your baseline plan changes (sleep, load, exercise quality), it becomes impossible to tell whether the peptide choice mattered.
Conclusion
When comparing bpc 157 vs tb 500, the practical takeaway is that these peptides are typically framed for different recovery “roles”: BPC-157 often as earlier support that helps you show up for rehab, and TB-500 often as a longer-horizon remodeling focus. Your results are most likely to reflect how well your training and healing phase match your expectations—and whether you measure progress instead of guessing.
Next step: Write down your current injury stage (early irritated vs remodeling), pick two measurable checkpoints for the next 4–6 weeks, and only then decide which peptide aligns better with your rehabilitation timeline and goals.
Discussion